


INJURY/ILLNESS REPORT
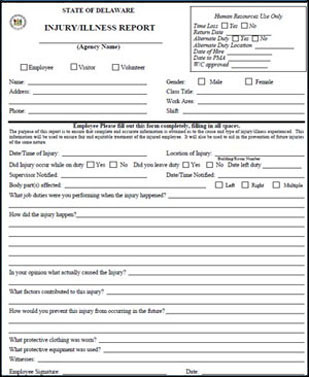

The following fields must be completed.
- Full first and last name of the employee filing the claim
- Current address and phone number of the employee filing the claim
- Date/time of injury
- Date/time supervisor was notified
- Signature of both employee and supervisor
**Incident Reports are not required and not part of this process.
Failure to complete the form in its entirety will delay the processing of the claim.
Please click on the Job Aid link for additional help with filling out the Injury/Illness Report.
Submitting Workers’ Compensation Claim